LA PRIMAVERA, É IL TEMPO DI DEPURARSI !
La primavera è come un nuovo inizio dopo l'inverno. È il momento perfetto per liberarsi dalle vecchie energie e abbracciare la freschezza e la vitalità che questa stagione porta con sé.
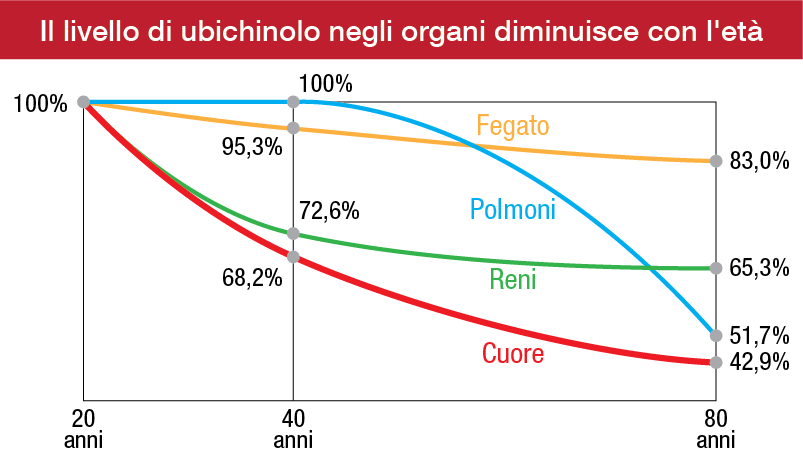
Con l'arrivo della primavera, molti di noi sentono il desiderio di liberarsi dalle tossine e dalle impurità (causate dal consumo alcolico, dai cibi grassi, zuccherati, fritti e alimenti trattati) accumulate nel corpo per sentirsi più leggeri e vitali. Anche se il nostro organismo ha già dei meccanismi di depurazione naturali grazie ai suoi organi, come il fegato, l'intestino e i reni, in questo periodo dell'anno possiamo dare loro una mano extra per migliorarne l'efficienza.
Il fegato è l’organo che ha bisogno di purificazione maggiormente nel nostro corpo a causa dell’accumulo di tossine. I ruoli principali del fegato sono:
- produrre la bile,
- favorire la trasformazione degli alimenti assorbiti,
- immagazzinare lo zucchero sottoforma di glicogeno.
Inoltre, ha un ruolo fondamentale sulla sintesi del colesterolo e dei trigliceridi, e sul metabolismo dei lipidi.
Come depurare il fegato in primavera con la fitoterapia?
Il cardo mariano, noto scientificamente come Silybum Marianum, contiene un potente principio attivo chiamato silimarina, che è ampiamente riconosciuto per i suoi benefici sulla salute del fegato.
La silimarina è particolarmente efficace nel migliorare la funzionalità epatica in diversi modi. Innanzitutto, aiuta nell'eliminazione delle tossine dall'organismo, svolgendo un ruolo chiave nella detossificazione. Inoltre, favorisce la rigenerazione delle cellule epatiche, contribuendo così a mantenere il fegato sano e funzionante.
Oltre a ciò, la silimarina può aiutare a proteggere il fegato dagli effetti dannosi di farmaci, fumo e altre sostanze tossiche, agendo come uno scudo protettivo per questo importante organo.
Il carciofo, conosciuto scientificamente come Cynara Scolymus, è ricco di micronutrienti e principi attivi che lo rendono estremamente utile per la salute epatica. La cinarina, l'acido clorogenico e i flavonoidi presenti nelle foglie del carciofo favoriscono la mobilizzazione dei grassi, l'escrezione della bile e la riduzione del colesterolo, contribuendo così alla salute del fegato.

Le foglie di carciofo sono particolarmente rinomate per la loro capacità di stimolare la diuresi e di eliminare le tossine dall'organismo. Anche se il loro sapore è amaro, i benefici che offrono sono notevoli: aiutano a ridurre il gonfiore addominale, favoriscono l'eliminazione dei liquidi in eccesso e rinvigoriscono la circolazione.
La radice di tarassaco, nota scientificamente come Taraxacum Officinale, è famosa per le sue proprietà depurative e antinfiammatorie. Le sue proprietà depurative e drenanti possono favorire il corretto funzionamento del fegato, stimolando la produzione di bile e agevolando il processo di eliminazione dalle tossine accumulate nell'organismo.
Gli estratti ottenuti dalle parti aeree del tarassaco hanno dimostrato di possedere diverse proprietà che favoriscono la bellezza e la salute della pelle. Questi estratti sono noti per le loro proprietà antimacchia, che possono contribuire a ridurre l'aspetto delle macchie cutanee e delle discromie, favorendo così un colorito più uniforme della pelle.

Il tarassaco può aiutare a stimolare l'attività renale, favorendo la produzione di urina e la rimozione delle scorie e delle tossine attraverso i reni. Questo può essere particolarmente utile per ridurre la ritenzione idrica e favorire la disintossicazione dell'organismo.
La colina, è una sostanza essenziale per il corpo umano che svolge diverse funzioni importanti, inclusa quella di facilitare il flusso della bile e favorire lo svuotamento della cistifellea. La sua azione consiste nel solubilizzare i grassi, aiutando così a prevenire il loro accumulo nel fegato.
Quando si tratta di proteggere e sostenere la salute del fegato, è utile considerare l'assunzione di piante epatoprotettrici, che possono essere utilizzate in combinazione per ottenere benefici sinergici. Noi possiamo integrare queste piante nella nostra dieta per proteggere il fegato da danni e stress, migliorando la sua funzionalità e favorendo la disintossicazione dell'organismo. Grazie alle loro proprietà, queste piante possono offrire un valido sostegno per mantenere il nostro fegato in salute e promuovere il benessere generale del nostro corpo.
Venneria, E. (2008). Valorizzazione dei prodotti ortofrutticoli tradizionali: effetti dell’efficacia antiossidante su modelli in vitro, ex vivo ed in vivo. Takkella, N., Konuri, A., Kishore, A., Rai, K. S., & Bhat, K. M. (2018). Role of Choline-Docosahexaenoic acid and Trigonella foenum graecum Seed Extract on Ovariectomy Induced Dyslipidemia and Oxidative Stress in Rat Model. Journal of Krishna Institute of Medical Sciences (JKIMSU), 7(1). DI SUPERSMART, I. C. Come ridurre la ritenzione idrica a livello dell’addome?. Omega, 2024, 01-11. Basnizki, Y., Zohary, D., & Mayer, A. M. (1992). Contenuto di cinarina e acido clorogenico nei semi germinanti di carciofo (Cynara scolymus L.). Journal of Genetics and Breeding, 46. GRASSO, C. S. N. F. LA SILIMARINA. De Fiore, R. Gli epatoprotettori proteggono il fegato?. Yang, Y., & Li, S. (2015). Dandelion extracts protect human skin fibroblasts from UVB damage and cellular senescence. Oxidative Medicine and Cellular Longevity, 2015. https://www.lombardinaturopata.it/2019/04/03/primavera-la-stagione-ideale-depurarefegato/#:~:text=Gli%20alimenti%20anticolesterolo%20per%20eccellenza,oilo%20extra%20vergine%20di%20oliva. Crocker, P. (2015). Succhi e centrifughe (Vol. 245). Newton Compton Editori.